
Laws and regulations imposed on clinics have nothing to do with patient care — and everything to do with limiting abortion access.
 In part one of this two-part series, I wrote about TRAP laws in Texas and across the country. The question of whether these sneaky, dangerous laws are Constitutional is headed to the U.S. Supreme Court, because they restrict women’s legal access to abortion by forcing abortion providers to adhere to regulations not required of any other medical professionals.
In part one of this two-part series, I wrote about TRAP laws in Texas and across the country. The question of whether these sneaky, dangerous laws are Constitutional is headed to the U.S. Supreme Court, because they restrict women’s legal access to abortion by forcing abortion providers to adhere to regulations not required of any other medical professionals.
To learn more about Targeted Regulation of Abortion Providers (TRAP) laws and other abortion restrictions in Michigan, I spoke with Renee Chelian, founder and CEO of Northland Family Planning Centers (NFP), and Lara Chelian, director of advocacy and development for NFP.
With three locations, NFP has been providing high-quality reproductive care, including abortion, since 1976. NFP and its staff adhere to medical standards written by doctors who perform abortions — standards specific to their field of medicine that are focused on protecting the health and safety of women. The fact is that surgical abortion is one of the safest procedures in the United States.
But because of TRAP laws and other regulations written by legislators, NFP and other providers are often forced to divert attention and funds from patient care, to jump through ridiculous hoops created by legislators who know absolutely nothing about the practice of medicine, Renee says.
These regulations aren’t about women’s health at all — they’re about closing abortion clinics. Their goal is to make it more difficult for us to practice, to continuously have us spend money on things we don’t need, and it can affect patient care because you start practicing to the regulations.
This is not to suggest that NFP is allowing itself to be distracted from giving women the best possible care. They have a 0.1% infection rate and adhere to the high standards established by the National Abortion Federation.
“We follow those standards voluntarily, because we want to stay on the cutting edge of the kind of medical care we offer,” Renee says.
But the reality is that TRAP laws and other Michigan state regulations force NFP to allocate resources to comply with rules that do not do anything to benefit patients.
 For example, House Bill 5711, a broad package of abortion restrictions, was signed into law by Gov. Rick Snyder at the end of 2012. The law required clinics like NFP to make significant facility renovations and administrative changes — costing NFP $250,000 in renovation costs alone.
For example, House Bill 5711, a broad package of abortion restrictions, was signed into law by Gov. Rick Snyder at the end of 2012. The law required clinics like NFP to make significant facility renovations and administrative changes — costing NFP $250,000 in renovation costs alone.
For example, NFP had to install scrub sinks, even though doctors don’t “scrub in” for abortions because they aren’t a sterile procedure; no incision is made. A surgical abortion is no more invasive than inserting an IUD — something that’s commonly done in a doctor’s office, where they don’t have to follow any of the regulations imposed on abortion providers.
NFP also had to remove beds from recovery rooms, because the state said beds were too close together, claiming that created an infection risk. “Our patients have always been sitting next to each other — in fact, they find a great deal of comfort in talking to each other,” Renee says.
In addition, Michigan abortion clinics were forced to meet the same criteria for heating and cooling system airflow and bacteria that’s required at hospitals. Again, because abortion doesn’t require an incision and infection rates are extremely low, extra measures to prevent contamination are not necessary.
Another required change was the lighting in procedure rooms. At NFP, inspectors decided the light level in the corners of procedure rooms — not where procedures are actually performed — wasn’t bright enough. The state claimed that the lighting was too dim to clean properly in the corners. But as Renee points out, many nurses have told them that NFP’s facilities are cleaner than any hospital they’ve worked in.
Of all the expensive and medically unnecessary modifications abortion care providers were required to make by the state of Michigan, perhaps the most ludicrous was the requirement for fire extinguisher signage. Renee explains.
One of the fire marshals came in and did a walkaround and said, ‘You don’t have a sign above your fire extinguisher.’I replied, ‘We have a fire extinguisher — people can see it.’ But the fire marshal said he wanted a sign six feet from the floor, and he wouldn’t pass us until every fire extinguisher had a sign.
We had the fire company we work with hang all these signs — even though they’re experts and said six feet wasn’t the right height. But when the fire marshal came back he pulled out a tape measure and said, ‘These aren’t six feet.’
Then he turned the sprinklers on in the furnace room, made a mess and basically said, ‘Get used to it.’
The regulations don’t end with facilities, either. Like other clinics, NFP was required to put together an entire book of written policies similar to those at hospitals, even though hospitals perform hundreds of different procedures, not just a handful. NFP spent six months taking its procedures and writing them into policy, which one staff member was paid to work on full time. Yet every time an inspector came in, they’d require revisions based on subjective opinions — not medical evidence.
None of these requirements do anything to benefit patients, as Lara explains.
These regulations are designed to have us keep spending money. In order to keep our doors open, we have to pass it on through fees and costs of abortion care. It’s literally costing us so much that we are having to put that cost back on the patient, and then it’s pricing women out of abortion care.
Not to mention that there are still costs involved in ongoing compliance, beyond the original $250,000 investment. And then there’s the cost of time taken away from the entire reason for NFP’s existence.
“Complying with all of these regulations keeps us from our number-one goal of taking the best possible care of patients,” Lara says. “None of this makes abortion safer for patients — it’s already safe. So the regulations are just intended to keep us from focusing on what’s really important for the overall health of women.”
It’s likely that more restrictions on reproductive care providers and abortion itself in Michigan will be considered this year, given the makeup of the Legislature and bills already in the hopper. And legislators dictating how medicine gets practiced is a troubling prospect for providers — and a dangerous one for women, Renee says.
If we make abortions more difficult to get, if we make it impossible for providers to stay open in this country, we will be facing a health crisis. Women aren’t going to turn back, and probably the same number of abortions will take place — just criminally, and less safely.
To stay up to date on the latest news on reproductive healthcare access in Michigan, join and follow the MI Lead women’s coalition.
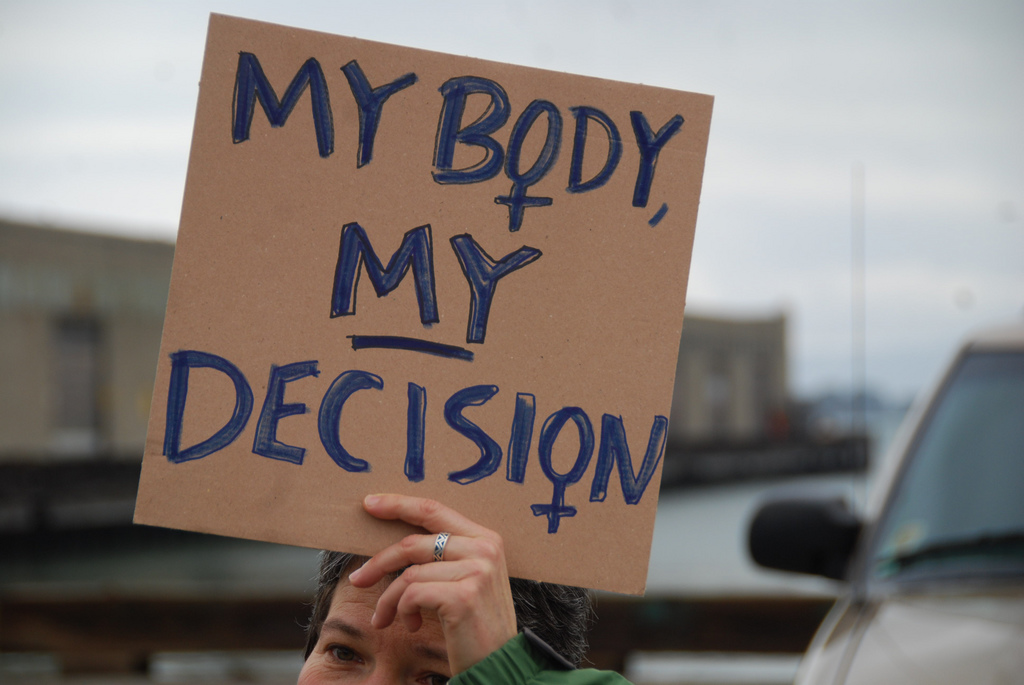
[Image credits: Top: Steve Rhodes via Flickr; bottom: Alex Proimos via Wikimedia Commons.]

